UTSW/BioTel EMS System
November 2014
EMS TB 14-007: Use of Medical Personal Protective Equipment (PPE) (PDF Here) (PPE Video)
Purpose:
To provide UTSW/BioTel EMS agency EMS Providers with guidelines for the proper use and removal/disposal of Personal Protective Equipment (PPE).
Background:
Recent events surrounding the confirmed cases of Ebola Virus Disease (EVD) in Dallas have prompted the need for refresher training and review of Department and EMS System Policies in the
proper use of PPE for all EMS Providers. The situation and official recommendations remain fluid. Moreover, there are many possible types of PPE equipment. The recommendations set forth in
this Training Bulletin are intended to be both safe and operationally feasible for EMS. The type of PPE components varies according to the mode of disease transmission. These PPE components
are deployed as part of four different, partially overlapping levels of “Isolation Precautions” for treating the patient and for interacting with the patient’s environment of care. These four categories
are: Standard, Contact, Droplet and Airborne Precautions. PPE is “what” is worn, while Isolation Precautions describe “how” the wearer uses this PPE when providing medical care. The procedure
for putting on (donning) and removing (doffing) PPE is also tailored to the specific type of PPE needed for each level of Isolation Precautions. A Buddy System with a second EMS Provider
observing the first EMS Provider during donning and doffing can help to ensure proper PPE use. The Buddy System shall be used whenever removing (doffing) PPE, if staffing allows.
Infection Control & Prevention Items Needed Prior to Patient Contact:
- Hand hygiene supplies
- • BioHazard bags & other infection control supplies (e.g. Lysol Professional Spray)
PPE Selection Recommendations:
NOTE: EMS Providers may always exercise clinical judgment to don a HIGHER level of PPE, especially RESPIRATORY Protection, if the clinical scenario warrants.
NOTE: This table does NOT include specific guidelines for disinfection of the environment of care (e.g. medical equipment, environmental surfaces, and ambulance surfaces, etc.)
Refer to UTSW/BioTel EMS TB 14-008, and to other BioTel and agency educational materials.
NOTE: Except for Air-Purifying Respirators (APRs), all equipment shall be disposed of after single use. APRs may be disinfected, as appropriate, per UTSW/BioTel EMS TB 14-008 and manufacturer recommendations.
PPE Component |
PPE Selection According to Clinical Scenario |
|
ALL Patient Encounters |
Patients with fever and/or other signs/symptoms, with any known or suspected infection, such as Ebola, Influenza & other viruses, Plague, Hepatitis B/C |
Patients with fever and/or other signs/symptoms & known or suspected infection with airborne-spread organism, such as TB, measles, or chickenpox; or unknown history |
|
“Standard Precautions” |
“Contact and Droplet Precautions” |
“Airborne
Precautions” |
DISPOSABLE GLOVES
|
YES
|
YES - DOUBLE |
YES - DOUBLE
|
GOWN (Impermeable or Fluid Resistant)
|
As needed
|
YES |
YES
|
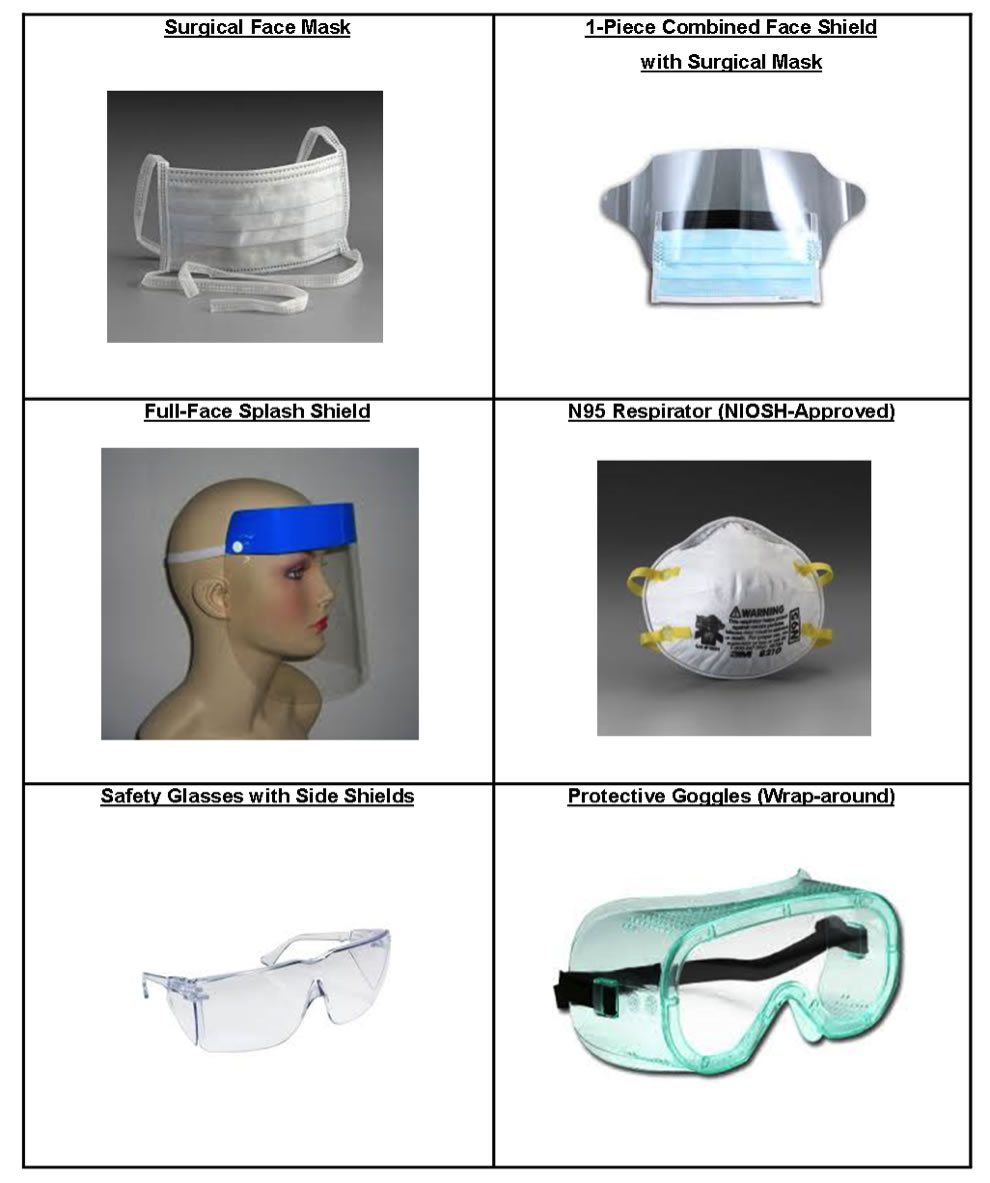
EYE + FACE PROTECTION OPTIONS:
- One-Piece Surgical Mask with Splash Shield (may be worn with 3M Safety Goggles), OR
- Full-Face Splash Shield and Surgical Mask or N95 (can be worn with 3M Safety Glasses), OR
- Green Safety Goggles and Surgical Mask or N95, as indicated (minimal exposed skin)
|
Option 1,
As needed |
Option 2 (preferred),
or Option 3
|
SEE BELOW |
RESPIRATORY PROTECTION |
|
|
|
- Standard Surgical Face Mask*
|
As needed |
YES, or higher
|
NO |
- N95 or N100 Respirator* (Must be worn with Eye Protection)
|
NO |
YES, especially if“High-Risk” or “Aerosol-Generating” Procedures (AGP†), e.g. CPR, Airway interventions |
YES |
(If available)
- Air-Purifying Respirator* (Must be worn with Eye Protection, unless full face) OR SCBA
|
NO |
NO
|
YES, especially if“High-Risk” or “Aerosol-Generating” Procedures (AGP†), e.g. CPR, Airway interventions |
SURGICAL FACE MASK for PATIENT? |
NO
|
YES |
YES
|
Special Circumstances:
- CPR, Airway Interventions and other procedures (known as “Aerosol Generating Procedures”, “AGP”†) may generate large volumes of patient body fluids (vomit, saliva, sputum, etc.)
- Performance of these procedures in a moving vehicle or under other relatively less controlled conditions increases the risk of EMS Provider exposure
- When possible, these procedures should be performed under safer conditions, such as: Stopped vehicle, or at the receiving hospital
- ADDITIONAL PPE that may be needed under these circumstances:
- Double GLOVES (additional pairs will be needed during doffing)
- Disposable boot covers or leg covers
- Disposable bonnets
Procedures – Putting On (Donning) PPE:
NOTE: A Buddy System with a second EMS Provider or other trained observer monitoring the first EMS Provider during both donning and (especially) doffing shall be used whenever possible.
Such a system can help to ensure proper PPE use and removal, and it has been shown to minimize the chance of a procedural breach and accidental exposure.
- “Lead Medic” (LM) will serve as Buddy for “Treating Medic” (TM), then vice versa
NOTE: Double Gloves should be worn if gross contamination is likely (e.g. due to a large volume of body fluids) or for other high-risk patient contacts. Wearing more than double gloves does NOT
provide more protection and may increase EMS Provider risk, because doing so complicates the doffing procedure.
- Remove personal items and perform Hand Hygiene
- Use ample alcohol-based hand gel and allow time for gel to be fully absorbed
- Tuck pants legs into socks or boots to facilitate donning and doffing with less risk of contamination
- Don Boot Covers
- Don waterproof or fluid impermeable Gown, tying at the waist and neck:
- Do not tie a tight knot that will make it hard to unfasten during doffing
- Don DOUBLE Gloves:
- Select outer glove size one size larger than inner gloves, if needed
- Gown cuff must be inside (under) the inner gloves, with no exposed skin
- Don Respiratory Protection (disposable mask or respirator):
- Standard surgical mask: routine, low-risk patients (“Standard Precautions”)
- N95: Patient with fever or other symptoms (“Contact and Droplet Precautions”)
- Air-Purifying Respirator: Patient with known or suspected high-risk infection with TB or similar airborne agent, or Unknown History (“Airborne Precautions”)
- Don Eye and Face Protection – based on PPE readily available as of October 2014:
- Green Wraparound Protective Goggles, OR
- Disposable Full-Face Splash Shield
- Can be worn with 3M Safety Glasses
- Cannot be worn with Green Protective Goggles
- Don Bonnet
- Buddy inspects PPE, front and back, for breaches or other defects
Procedures – Removing (Doffing) PPE:
- Most Health Care Provider exposures occur during PPE removal (doffing)!
- To minimize exposure risk, PPE must be removed carefully and in the proper sequence.
- EMS Providers shall use a Buddy System during doffing, whenever possible:
- “Lead Medic” (LM) serves as “Buddy” during “Treating Medic” (TM) doffing;
- TM then dons fresh hospital Standard Precautions and serves as “Buddy” during LM doffing.
- Do NOT touch “dirty” surfaces with “clean” hands/gloves.
- DO NOT touch “clean” surfaces with “dirty” hands/gloves.
- Do NOT touch your eyes, nose or mouth while wearing PPE or during PPE removal, until AFTER the final Hand Hygiene and soap-and-water cleansing have been performed.
- Discard gloves and perform Hand Hygiene at any point in the process or between steps, if gloves become inadvertently contaminated.
- Any procedure breach during doffing must be reported as soon as possible to the EMS Field Supervisor.
- Equipment needed:
- Lysol Spray: bring in to E.D. with patient!
- Biohazard bags/receptacle
- Clean, disposable gloves
- Hand hygiene supplies
- 1 set or 1 package of HOSPITAL “Standard Precautions” Disposable PPE
- Disposable gloves (at least two or three pairs per team)
- Gown
- Standard Surgical Mask (preferably with attached splash shield or other eye protection)
- Chair, if available
➢ Start with both Medics in full PPE (including double gloves), after transfer of patient care.
- LM sprays TM from the waist down with Lysol (attention: bottom of boot covers, exposed trouser legs, etc.)
- TM removes boot covers, trying NOT to touch the inside of boot covers or pants legs –› Biohazard disposal, as each one is removed
- It may be necessary to sit or to lean against a wall, but do NOT cross legs while removing boot covers
- TM removes OUTER gloves (without contaminating inner gloves or skin) –› Biohazard disposal
- LM unfastens TM gown, touching it only in the rear and as little as possible
- TM removes gown AND INNER gloves, touching only the inside of the gown and gloves –› Biohazard disposal:
- Roll and bundle the gown during removal, creating a manageable bundle
- Bend slightly forward to keep the gown from touching clothing
- Avoid contaminating bare skin with gloved hands
- TM performs Hand Hygiene for at least 20 seconds
- Allow hand gel to be fully absorbed and hands to dry as much as possible
- TM dons TWO pairs of clean, disposable gloves
- TM uses only ONE hand to remove bonnet –› Biohazard disposal
- Lift off to the side, not towards the face
- TM uses the OTHER hand to remove goggles or face shield –› Biohazard disposal
- Do not touch inside of goggles or face shield
- TM removes only OUTER gloves without contaminating inner gloves –› Biohazard disposal
- TM removes mask or respirator à Biohazard disposal
- Grasp mask with one hand and straps with the other hand, lifting away from the face while actively exhaling
- TM removes INNER gloves, without contaminating bare hands –› Biohazard disposal
- TM performs thorough Hand Hygiene
- TM dons HOSPITAL Standard Precautions PPE
- Gown
- Mask (Standard surgical mask with face shield, or equivalent)
- Disposable gloves (one or two pairs)
- TM wipes Lysol can with disposable hand sanitizing wipe or equivalent –› Biohazard disposal
- TM should remove outer gloves (if worn), or should remove the single pair of gloves, perform Hand Hygiene and don clean gloves, if needed, after this step (e.g. if the Lysol can is visibly soiled)
- The entire Doffing procedure now repeats from Step #1 for the LM, except that the TM (in Standard Precautions) is now the “Buddy” for the LM during his/her doffing procedure
- When the LM has been fully doffed, he/she performs Hand Hygiene and dons one pair of disposable gloves
- LM unfastens TM’s gown for TM’s removal of Standard Precautions PPE
- TM removes gown, mask, then gloves without contaminating skin or mucous membranes
- Both Medics perform Hand Hygiene, and wash hands and all at-risk skin surfaces with soap and water
- Dispose of PPE at the hospital, if possible, as advised by facility staff
Steps To Take In the Event of Possible EMS Provider Contamination (Refer to the UTSW/BioTel TB 14-008 Decon):
- If blood, body fluids, secretions, or excretions from a patient with suspected Ebola or other communicable disease come into direct contact with one’s skin or mucous membranes, stop working as soon as
possible and wash the affected skin surfaces thoroughly with soap and water.
- Report the exposure as soon as possible to your EMS Supervisor for follow-up.
- Follow all other EMS Agency-specific guidelines and policies regarding potential infectious disease and bloodborne pathogen exposures.
SUMMARY of Recommendations:
- Good hand hygiene is the single most important means to prevent infection spread!
- EMS Providers shall wear appropriate PPE and apply appropriate isolation precautions when entering the scene, and shall continue to wear PPE until no longer in contact with the patient or his/her environment.
- Gloves should be replaced when torn or visibly contaminated.
- EMS Providers should limit the number of surfaces touched while wearing PPE & should keep hands away from their face, as much as possible.
- EMS Providers shall not eat, drink, or use tobacco products during patient contact.
- PPE should be carefully removed in the proper sequence, without contaminating one’s eyes, mucous membranes, or clothing with potentially infectious substances.
- EMS Providers should remove PPE as soon as possible, when not involved in patient care, transferring patient care, or disinfecting the ambulance.
- PPE should NOT be worn in BioTel or in areas where it is not needed (e.g. completing documentation at Emergency Department Nurses’ Station, or printing the ePCR, etc.).
- PPE should be disposed of properly in a red “Biohazard” medical waste container, or by double-bagging, labeling and maintenance in a secure location until appropriate disposal can be performed.
- Reusable PPE shall be cleaned and disinfected according to the manufacturer’s reprocessing instructions and EMS agency policies/procedures.
For ANY questions or concerns, contact your EMS Supervisor or BioTel immediately.
CDC Resources*:
http://www.cdc.gov/vhf/ebola/hcp/interim-guidance-emergency-medical-services-systems-911-public-safety-answering-points-management-patients-known-suspected-united-states.html
http://www.cdc.gov/vhf/ebola/pdf/ems-checklist-ebola-preparedness.pdf
http://www.cdc.gov/vhf/ebola/pdf/checklist-patients-evaluated-us-evd.pdf
http://www.cdc.gov/vhf/ebola/pdf/ppe-poster.pdf
http://www.cdc.gov/vhf/ebola/hcp/environmental-infection-control-in-hospitals.html
http://www.cdc.gov/hicpac/2007IP/2007ip_part2.html#e
http://www.cdc.gov/vhf/ebola/hcp/infection-prevention-and-control-recommendations.html
http://www.cdc.gov/HAI/ppt/ppe/PPEslides6-29-04.ppt
*Accessed 6 November 2014
†AGP: Aerosol-Generating Procedure
“Although there are limited data available to definitively define a list of AGPs, procedures that are usually included are Bilevel Positive Airway Pressure (BiPAP), bronchoscopy, sputum induction, intubation and
extubation, and open suctioning of airways.” CPR is not specifically included on the list as an AGP; however, endotracheal intubation may be performed during CPR.
PICTORIAL GLOSSARY of PPE
(Representative Examples, as of October 2014)